
Starting Hormone Replacement Therapy (HRT) is often a turning point. You finally get relief from the hot flushes, the brain fog lifts, and you start to feel like yourself again. But for some women, this relief is interrupted by an unwelcome surprise: bleeding on continuous HRT.
If you are on a “bleed-free” (continuous combined) HRT regimen, seeing blood in your underwear can be confusing and worrying. You might think, “I thought my periods were over?” or “Is the HRT not working?”
First, please know that you are not alone. Irregular bleeding on HRT treatment is one of the most common reasons women contact my clinic. While it is often a nuisance side effect as your body adjusts, it can sometimes signal that your hormone regime needs tweaking or that a gynaecological check-up is due.
In this detailed guide, we will explore the mechanisms behind bleeding after menopause on HRT, distinguish between “settling in” bleeding and abnormal bleeding, and outline the steps we take to fix it according to British Menopause Society (BMS) guidance.
What is Continuous HRT?
To understand why bleeding happens, we first need to look at how your HRT works.
If you are postmenopausal (defined as having had no natural period for 12 months or more), you are typically prescribed postmenopausal treatment or continuous combined HRT. This regimen delivers a daily dose of two hormones:
- Estrogen: To manage symptoms and protect bone/heart health.
- Progesterone (or progestogen): To protect the lining of the womb (endometrium).
Unlike “sequential” HRT, which includes a planned break to induce a monthly bleed, continuous HRT is designed to keep the womb lining thin and stable, resulting in no bleeding at all. However, achieving that perfect stability can sometimes be a balancing act.
The “Settling In” Period: When Bleeding is Normal
If you have recently started continuous HRT, or if you have recently increased your estrogen dose, some bleeding is actually expected.
The BMS guidelines state that unscheduled bleeding is common in the first 3 to 6 months of starting or changing a simplified HRT regimen. This is known as the “settling in” phase.
Why does this happen? When you reintroduce estrogen to a postmenopausal body, the receptors in the womb lining “wake up.” The progesterone part of your HRT is there to keep the lining thin, but it takes time for the receptors to down-regulate and for the lining to become dormant again. During this tug-of-war, you may experience:
- Light spotting.
- Brown discharge.
- Intermittent cramping.
If you are within this 6-month window, and the bleeding is light and not associated with pain or bleeding after sex, we often recommend waiting it out. However, if the bleeding is heavy or persists beyond 6 months, it becomes classified as abnormal bleeding on hormone replacement therapy and requires investigation.
Common Causes of Bleeding on Continuous HRT
Once we are past the initial settling-in period, or if bleeding starts suddenly after years of stability, we need to find the cause.
1. Atrophic Changes (Genitourinary Syndrome of Menopause)
Paradoxically, the most common cause of vaginal bleeding on HRT UK specialists see is not too much hormone, but arguably not enough locally.
Even when taking systemic HRT, the vaginal tissues can remain thin and fragile (atrophic). This condition, known as Genitourinary Syndrome of Menopause (GSM), makes the tissues prone to tearing and bleeding during daily activities or intercourse.
- The Clue: The bleeding is often bright red, follows exercise or sex, and may be accompanied by soreness or stinging.
- The Fix: Adding localized vaginal estrogen (pessaries or creams) alongside your HRT patches or gels usually resolves this.
2. Progesterone Intolerance or Insufficiency
This is a frequent culprit for postmenopausal bleeding on HRT.
To keep the womb lining thin, the dose of progesterone must be high enough to “oppose” the estrogen. If your estrogen dose is high (to control flushes) but your progesterone dose is standard, the estrogen may stimulate the lining just enough to make it unstable and shed.
- The “Leak” Effect: Imagine a bucket being filled with water (estrogen). If the lid (progesterone) isn’t tight enough, water will occasionally splash out.
- Absorption Issues: We also see this in women who do not absorb progesterone well through the gut (capsules) or skin (patches).
3. Compliance Issues
Hormone levels drop very quickly if a dose is missed.
- Forgetting to change a patch or take a pill.
- Patches peeling off after a shower or swim.
- Taking supplements that interfere with hormone absorption. Any dip in hormone levels can trigger a “withdrawal bleed,” similar to the end of a pill packet.
4. Structural Causes: Polyps and Fibroids
Sometimes, the bleeding is unrelated to the hormones themselves but is caused by a structural issue that the hormones might be highlighting.
- Polyps: These are soft, fleshy growths inside the womb or on the cervix. They are very vascular and bleed easily. Estrogen can sometimes encourage them to grow.
- Fibroids: These are muscular knots in the womb wall. While they usually shrink after menopause, HRT can sometimes maintain them, leading to irregular bleeding on HRT treatment.
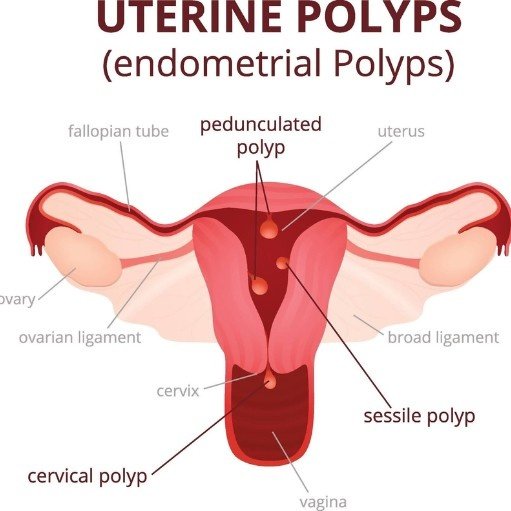
Uterine Polyps
5. Endometrial Pathology
We must always consider the serious causes. Postmenopausal bleeding on HRT is a red flag symptom for:
- Endometrial Hyperplasia: A thickening of the womb lining. This is a pre-cancerous condition often caused by “unopposed” estrogen (not enough progesterone protection).
- Endometrial Cancer: While less likely, any bleeding after menopause must be investigated to rule this out.
Investigating the Bleeding: The “Check-Up”
If you have bleeding on continuous HRT that has lasted longer than 6 months, or if it is heavy/painful, you should not just “put up with it.” You need a clinical assessment.
At a specialist clinic or your GP, the pathway is systematic:
Step 1: History and Examination We will ask about your HRT regimen (doses, brands, timing) and your bleeding pattern. A pelvic exam allows us to check for vaginal atrophy, cervical polyps, or ectropion (cells on the cervix surface).
Step 2: Transvaginal Ultrasound (TVS) This is the most important initial test. We look at the Endometrial Thickness (ET).
- On Continuous HRT: The lining should ideally be thin (usually below 4mm or 5mm, though guidelines vary slightly depending on individual risk).
- If the lining is thin and smooth, the bleeding is likely due to atrophy or hormonal imbalance (progesterone insufficiency).
- If the lining is thickened or irregular, further testing is needed.
Step 3: Hysteroscopy and Biopsy If the scan shows a thick lining or a polyp, we can refer you for a hysteroscopy (a tiny camera into the womb). This allows to take a sample (biopsy) to check the cells. This is the definitive way to rule out hyperplasia or cancer.
Managing and Treating the Bleeding
Once we know the cause, we can fix it.
Scenario A: The Scan is Normal (Thin Lining)
If the womb is healthy, the bleeding is likely hormonal or atrophic. We may:
- Treat Atrophy: Prescribe Vagifem or Ovestin cream.
- Adjust the Progesterone: The BMS guidelines suggest increasing the progestogen dose.
- If you take oral progesterone (e.g., Utrogestan) 100mg, we may increase it to 200mg or suggest taking it vaginally (off-licence use) to improve absorption.
- If you are on patches, we may switch you to a separate estrogen and progesterone regimen to have more control over the doses.
- Switch to the Mirena Coil (IUS): This is often the “gold standard” for bleeding control. The Mirena releases progesterone directly into the womb, thinning the lining very effectively while allowing you to take the estrogen you need.
Scenario B: The Scan Shows a Polyp
We can refer for the polyp to be removed (polypectomy). This is a simple day-case procedure. Once removed, the bleeding usually stops completely.
Scenario C: The Scan Shows Thickened Lining (Hyperplasia)
If the biopsy confirms hyperplasia, the management is not “one size fits all.” It is decided strictly based on the biopsy results (the type of cells found) and an individual risk assessment
A Note on Other Hormones
Occasionally, women using Testosterone Therapy for Women may worry this is contributing to bleeding. Testosterone does not generally cause uterine bleeding, as it does not stimulate the endometrial lining in the same way estrogen does. However, your specialist will review your full hormone profile during your assessment.
Summary: When to Seek Help
Bleeding on continuous HRT is rarely an emergency, but it is always a signal from your body that requires interpretation.
You should book an appointment if:
- You have been on HRT for more than 6 months and bleeding persists.
- Bleeding starts suddenly after a long period of being bleed-free.
- The bleeding is heavy (clots or flooding).
- You experience bleeding after sex (postcoital bleeding).
- You have pelvic pain.
Most cases of vaginal bleeding on HRT UK wide are solved by tweaking the balance of your hormones—often by increasing progesterone or switching to a Mirena coil. You do not necessarily have to stop HRT; we just need to find the right regimen for your body.
Book appointment confidential bleeding check If you are struggling with irregular bleeding on HRT, let us help you regain control. Book a specialist consultation today for a full review and scan.
Frequently Asked Questions
Is bleeding on continuous HRT normal?
It is considered “normal” or expected during the first 3 to 6 months of starting treatment. This is the body adjusting. However, bleeding that continues beyond 6 months, or starts after you have been stable for a long time, is considered abnormal and should be checked.
Can stress cause bleeding on HRT?
No. Stress can affect periods in younger women by stopping ovulation, but in postmenopausal women on HRT, bleeding is usually mechanical (atrophy/polyps) or hormonal (absorption issues). It should not be dismissed as stress.
Does increasing estrogen stop bleeding?
Usually, it is the opposite. Increasing estrogen without increasing progesterone can stimulate the womb lining and cause bleeding. To stop bleeding, we usually need to increase the progesterone or reduce the estrogen.
Can I just stop my HRT to stop the bleeding?
Stopping HRT will usually cause a “withdrawal bleed” (like the end of a pill packet) a few days later. After that, the bleeding should stop, but your menopausal symptoms (flushes, mood changes) will likely return. It is better to consult a specialist to adjust the HRT rather than just stopping.
Why am I bleeding on patches but didn’t on tablets?
Absorption varies hugely between women. You may have been absorbing the tablet progesterone well, but not absorbing the patch progesterone effectively, leading to a thin/unstable lining. Switching delivery methods (e.g., to a Mirena coil) often solves this.
Sources & Guidelines
- British Menopause Society (BMS): Management of Unscheduled Bleeding on HRT https://thebms.org.uk/publications/bms-guidelines/management-of-unscheduled-bleeding-on-hormone-replacement-therapy-hrt/
- NHS: Hormone Replacement Therapy (HRT) Side Effects https://www.nhs.uk/conditions/hormone-replacement-therapy-hrt/side-effects/
- NICE Guideline [NG23]: Menopause: diagnosis and management https://www.nice.org.uk/guidance/ng23
- Women’s Health Concern: HRT and Bleeding https://www.womens-health-concern.org/help-and-advice/factsheets/hrt-know-the-risks/





